IMÁGENES CIENTÍFICAS
Ahmed valve dislocation secondary to contusion
Fernando Godina, María A Piedrahitab, Catalina Betancurb, María A. Orregob
a Grupo de Investigación y Salud Ocular, Departmento de Oftalmología, Universidad El Bosque, Unbosque, Bogotá D.C., Colombia.
b Escuela de Medicina, Universidad CES, Medellín, Colombia.
Received: Septiember 15th, 2022.
Aprobado: October 17th, 2022.
Corresponding author
María A. Piedrahita, MD
Escuela de Medicina
Universidad CES
Cl 10A #22 - 04, El Poblado
Medellín, Colombia.
mapipiedrahita@gmail.com
Oftalmol Clin Exp (ISSNe 1851-2658)
2022; 15(4): e505-e507.
Refractory glaucoma is defined as an uncontrolled intraocular pressure (IOP) with evidence of optic nerve or visual file deterioration despite optimal doses of antiglaucoma medication. Therefore, glaucoma drainage devices, such as the Ahmed glaucoma valve (AGV), represent a valuable therapeutic alternative in these cases1. Although AGV safety has been widely demonstrated, important complications include hypotony, excessive capsule fibrosis, tube exposure, endophthalmitis and strabismus1-4. Some series have shown that the most frequent AGV complications are those related to the tube, which include tube exposure, obstructions, migration, and tube-corneal touching5.
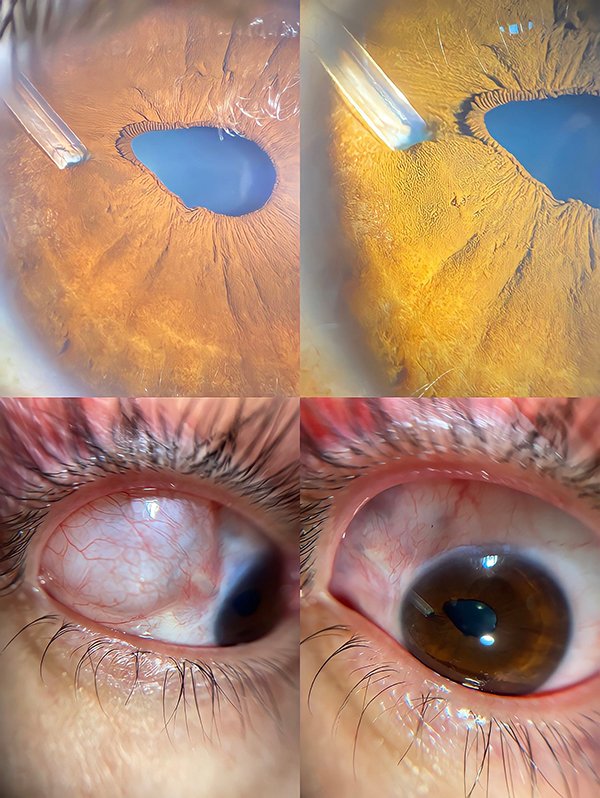
We present a 40-year-old man, who presented at a tertiary care unit with a history of blunt trauma to the right eye (RE) three years ago in a football game with a ball. He developed post-traumatic uveitis with an acute increase in IOP. He required surgical management with an AGV. He presents persistent pain and foreign body sensation in his RE after trauma from falling from a bicycle a month ago. Slit-lamp examination showed dislocation of the temporal-superior AGV with a conjunctival cyst, discoric pupil secondary to pulling due to the valve at the 9-10 meridian. IOP was within limits in both eyes; Fundus examination was adequate.
Tube exposure is a rare complication of AGV6. Although there have been case reports regarding spontaneous tube extrusion as reported by Grave et al.2, extrusion related to scleral patch graft thinning and conjunctival erosion like Mansoori et al.7 describe and corneal perforation due to exteriorization of the tube secondary to trauma in a pediatric patient reported by Kumar et al.8, dislocation due to blunt trauma is still rare. Considering this an uncommon case, it is crucial to recognize the findings in these images and the patient's symptoms and history to make a prompt diagnosis and provide adequate treatment.
Slit Lamp photographs of the right eye. Slit Lamp examination revealed dislocation of the temporal-superior AGV. (A-B) Pulling of the iris causing pupillary dyscoria. (C-D) Conjunctival cyst and dislocation of the AGV.
References