TÉCNICA QUIRÚRGICA
Transforming a vitrectomy hand-piece into a retinal substance injecting device
Juan Martín Giambruni, David Diamint, Gonzalo Gossn, Quiniano Chávez-Raraz
Retinal Service, Hospital Italiano de Buenos Aires, Buenos Aires, Argentina.
Received: June 29th, 2022.
Approved: August 15th, 2022.
Corresponsal author
Dr. Gonzalo Gossn
Hospital Italiano de Buenos Aires
Pres. Tte. Gral. Juan Domingo Perón 4190
(C1199) Buenos Aires, Argentina
+54 9 2215 65-1851
gonzalo.gossn@gmail.com
Oftalmol Clin Exp (ISSN 1851-2658)
2022; 15(3): e378-e381.
Conflicts of interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Abstract
Objective: To describe a procedure for converting a vitrectomy hand-piece into an injecting retinal substance device.
Surgical technique: We used a 23-gauge vitrectomy hand-piece with a lateral vent. Both tubes were disconnected, and their connection was changed in order to reverse liquid circulation, keeping the tube that had the connector. The cannula was cut in order to obtain a final extension of 6 to 8 centimeters in length. It was connected to the aspiration hole, whereas the other extreme was connected to a 5 centimeter syringe containing a dye.
The assistant surgeon injected the dye while the surgeon held the vitrectomy modified hand-piece in his right hand. The injected dye spread to the lateral space, slowly avoiding a retinal jet trauma.
Conclusion: We describe a standardized procedure for modifying a vitrectomy hand-piece. It can be used for injecting retinal substances and therefore avoiding retinal jet stream damage.
Key words: cannula, epiretinal membranes, hand-piece, injection, internal limiting membrane.
Transformación de una pieza de mano de vitrectomía en un dispositivo de inyección de sustancias en la retina
Resumen
Objetivo: Describir un procedimiento para convertir una pieza de mano de vitrectomía en un dispositivo para la inyección de sustancias retinales.
Técnica quirúrgica: Se utilizó una pieza de mano de vitrectomía de calibre 23 G con agujero lateral. Se desconectaron ambos tubos y se cambió su conexión para invertir la circulación del líquido manteniendo el tubo que tenía el conector. Se cortó la cánula para obtener una extensión final de 6 a 8 centímetros de longitud. Se conectó al orificio de aspiración mientras que el otro extremo se empalmó a una jeringa de 5 centímetros que contenía un colorante. El ayudante de cirugía inyectó el colorante mientras que el cirujano sostenía la pieza de mano modificada en su mano derecha. El colorante inyectado se extendió de forma lateral lentamente, evitando el traumatismo de la retina.
Conclusión: Describimos un procedimiento estandarizado para modificar una pieza de mano de vitrectomía. Puede utilizarse para inyectar sustancias en la retina y evitar el daño mecánico por la inyección del fluido.
Palabras clave: cánula, membranas epirretinales, pieza de mano, inyección, membrana limitante interna.
Transformação de uma peça de mão de vitrectomia em um dispositivo de injeção de substância retiniana
Resumo
Objetivo: Descrever um procedimento para converter uma peça de mão de vitrectomia em um dispositivo de injeção de substância retiniana.
Técnica cirúrgica: Foi utilizada peça de mão de vitrectomia 23 G com orifício lateral. Ambos os tubos foram desconectados e sua conexão foi alterada para reverter a circulação do líquido, mantendo o tubo que possuía o conector. A cânula foi cortada para obter uma extensão final de 6 a 8 centímetros de comprimento. Foi conectado à porta de aspiração enquanto a outra extremidade foi conectada a uma seringa de 5 centímetros contendo um corante. O assistente cirúrgico injetou o corante enquanto o cirurgião segurava a peça de mão modificada na mão direita. O corante injetado se espalhou lentamente lateralmente, evitando trauma na retina.
Conclusão: Descrevemos um procedimento padronizado para modificar uma peça de mão de vitrectomia. Ele pode ser usado para injetar substâncias na retina e evitar danos mecânicos da injeção de fluido.
Palavras-chave: cânula, membranas epirretinianas, peça de mão, injeção, membrana limitante interna.
Introduction
Chromovitrectomy consists in introducing dyes into the ocular fundus to improve the visualization of retinal structures during the vitrectomy surgical procedure1. Its reported advantages are related to its capacity to enhance a surgeon’s ability in managing the epiretinal membranes (ERM) and the internal limiting membrane (ILM). However, chromovitrectomy can induce complications directly associated with dye toxicity2-4, or secondarily related to the injection procedure itself5-6, where a mechanical trauma can be produced to the retina associated with the jet stream generated during the injection. To avoid this, there is a cannula called SideFlō (MedOne Surgical, Sarasota, USA)7; however, it adds an extra cost to the surgery and, mainly, it is not always available in developing countries.
Our group has been working since 2010 on trying to find a simple solution to inject substances during vitreo-retinal surgery. Considering that the vitrectomy hand-piece has a lateral vent, we thought it could provide better control during substance injection. By performing a few modifications on this device, it can be used for injecting substances during vitreo-retinal surgery. The purpose of this work is to present a detailed description of our developed technique.
Technique
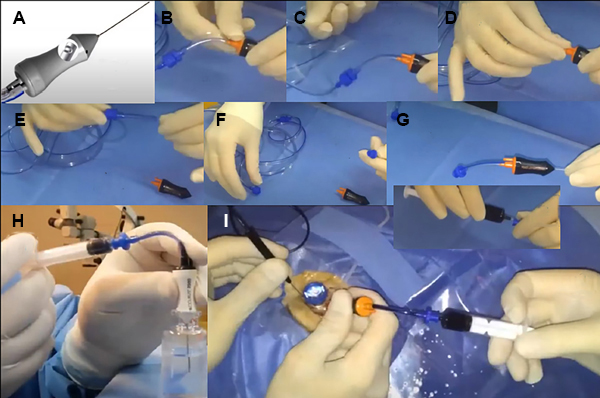
The procedure will be described, step by step, in the following paragraphs (also see Fig. 1, which is a composite made up of 10 pictures).
1. The vitrectomy hand-piece, used for cutting and aspiration, contains a lateral vent on its distal extreme, and two tube connectors on the other one (Fig. 1A). A new vitrectomy hand-piece can be used or, as is usually the case for us, a used blunt blade trocar (sterilized) vitrectomy hand-piece. It can be used with different vitrectomy hand-piece: 20 gauge (G), 23G, 25G, or 27G. In our case we are showing the technique with a vitrectomy 23G hand-piece.
2. The connection of the tubes for reversing liquid circulation must be changed (we want to inject fluids, not aspirate them). To do that, take both tubes off the hand-piece: the pneumatic control tube, and the aspiration tuve (Figs. 1B-E).
3. Keep the tube that has the connector, and cut the cannula, in order to obtain a final extension of 6 to 8 centimeters (cm) in length (Figs. 1F-G).
4. Connect it to the aspiration hole. The other extreme must be connected to a 5 cm syringe containing the dye (Fig. 1H).
5. After this, the cannula is ready to be used. The injected fluid spreads to the lateral space (Fig. 1I). Picture J of figure 1 shows how the procedure is done with the help of an assistant surgeon who is injecting the dye (trypan blue in this case), while the surgeon holds the vitrectomy modified hand-piece in his right hand.
Figure 1. Steps for converting a 23-gauge vitrectomy hand-piece into a cannula for injecting substances. This figure shows the technical procedure, step by step (a detailed description is in the text).
Discussion
The injection of substances during vitreo-retinal surgery entails an increased risk of retinal injury associated with the axial jet effect. Our group has developed a simple technique based on different vitrectomy hand-pieces available to any surgical team. Since this device has only one lateral vent (for cutting and aspiration), it can be rotated 360 degrees if a more extensive area needs to be covered with the dye. These substances can be injected slowly, with great control. This way we can inject dyes and other substances, such as perfluorocarbon liquid, without the risk of producing jet stream mechanical damage. This aspect is especially important when the injection is close to the macula. With our technique, we avoid the possibility of ejecting dye at high velocity directly pointed to the retina, which can happen due to a defective syringe, or when an inexperienced surgical assistant applies excessive while manipulating the syringe.
We are using a known surgical tool. Every retinal surgeon is familiarized with its ergonomical aspects. We are just modifying its function in order to inject substances instead of its standard functions of cutting and vitreous aspiration. Another important aspect is the cost, which is zero. This is because we are using a surgical device (a vitrectomy hand-piece) that is already included in the list of vitrectomy surgical supplies. Even so, a sterilized used one with a blunt blade trocar can be useful, because we do not have to use the cutting mechanism of the hand-piece. This is an important aspect for developing countries and/or places in the world where surgical supplies are imported and sometimes face different limitations, such as difficulties in international distribution, economical aspects, as well as political issues.
Injecting dye substances with the bomb of some vitrectomy equipment and their vitrectomy hand-piece is also a possibility. However, it is not always available to all surgeons. A very good commercial option for injecting substances is the SideFlō cannula, which has an oval side port near the tip of the cannula, and four holes placed along the outside of the tube, to eliminate the axial jet. Also, the SideFlō design has proved to have an enhancing passive outflow venting, as Toygar et al have published7. Our group has proved it is very good. However, we do not always have the possibility to use it frequently due to importing and commercial issues/policies. An interesting and similar technique was published in 2015 by Hahn, performing another procedure set-up and injecting triamcinolone acetonide or indocyanine green8.
In conclusion, in this work we described a technique to perform some modifications on the vitrectomy hand-piece, turning it into a device to inject substances during retinal surgery in a safe and controlled fashion. We hope that this technique can be useful for other retinal surgeons in the world, especially in developing countries.
References