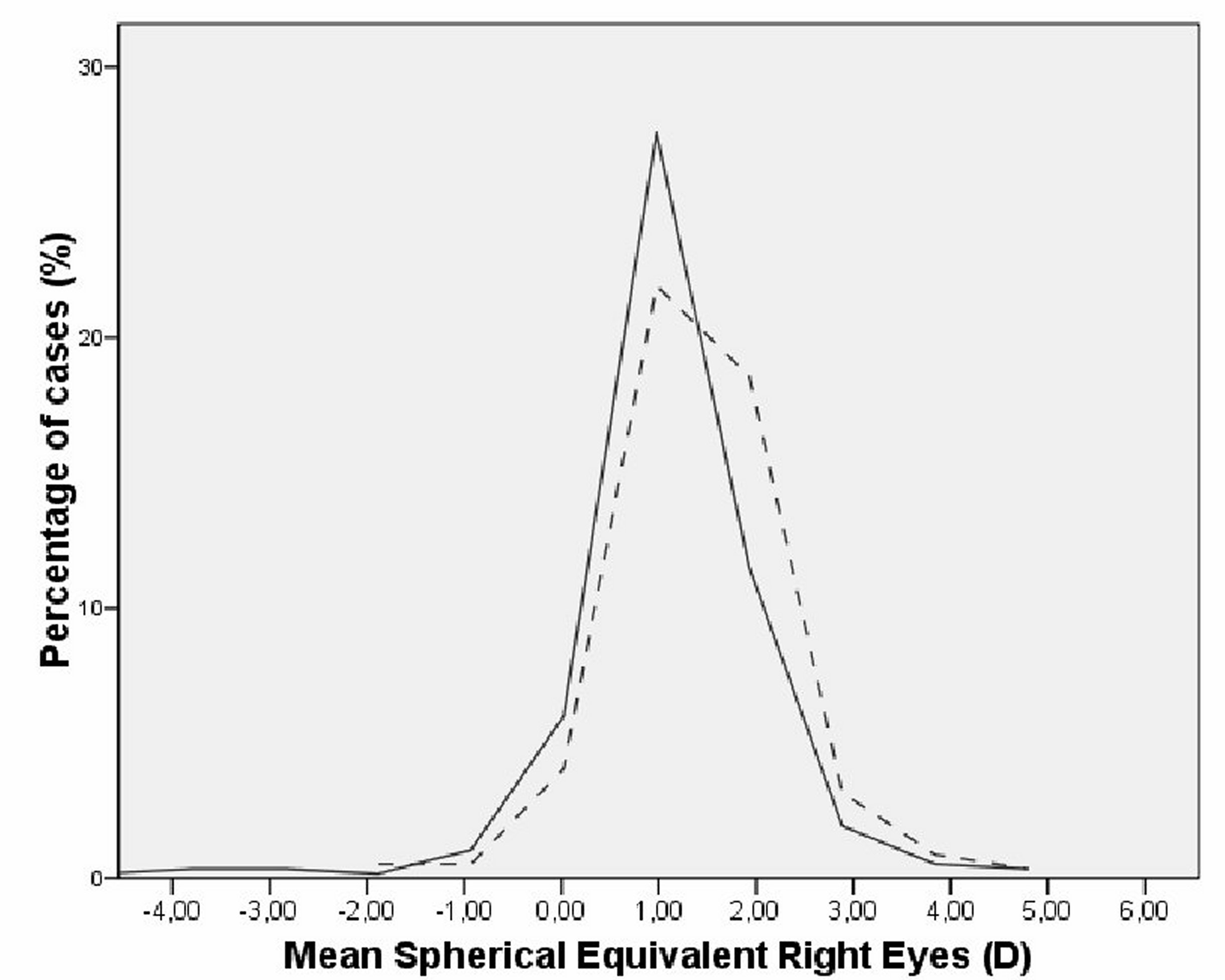
Figure 1. Histogram showing the distributions of spherical equivalent refractions, initially (dashed line) and after 5 years (solid line), showing slight loss of hyperopia without significant changes in myopia prevalence.
Low prevalence of myopia in children from a rural population in Marcos Juárez, Argentina
Ignacio Magnettoa, Omar Magnettoa, Agustín Magnettoa, Rodrigo M. Torresb, Rafael Iribarrenc
a Dr. Magnetto Ophthalmological Center, Marcos Juárez, Córdoba, Argentina.
b ROMAT, Colonia Avellaneda, Entre Ríos, Argentina.
c Dres. Iribarren Eye Consultants, Buenos Aires, Argentina.
Received: August 8th, 2021.
Aproved: November 25th, 2021.
Corresponding author
Dr. Rafael Iribarren
Arenales 981
(1061) Buenos Aires, Argentina
+54-911-5147-9312
rafairibarren@gmail.com
Oftalmol Clin Exp (ISSN 2718-7446)
2022; 15(1): e31-e39.
Abstract
Purpose: This study was developed to evaluate the prevalence and progression of myopia in children living in a rural area of Argentina.
Methods: This was a prospective school-based cohort study of refractive error. Children attending all schools in Marcos Juarez were examined first at school entrance and 5 years later (ages 11-12). The spherical equivalent refraction (SER) was obtained with cycloplegia.
Results: In 2013, 347 children were examined and 283 of these were available 5 years later (81%). At follow-up mean age was 11.84 ± 0.36 years. The mean SER was +1.36 ± 0.83 D in 2013 and decreased significantly to +1.07 ± 1.03 D in 2018 (an overall shift of -0.30 D, p<0.001). The prevalence of myopia < -0.50 D was low (2.12% in 2013 and 3.53% in 2018), and there were no cases of high myopia < -5.00 D in either period. The prevalence of hyperopia (> +2.00 D) decreased from 15.55% in 2013, to 9.54% in 2018, while the prevalence of emmetropia and low hyperopia (-0.50 to +2.00 D) increased with follow-up (82.68% in 2013 to 86.92% in 2018). There was a very low incidence of myopia in five years (1.44%).
Conclusion: A low prevalence and incidence of myopia was detected in a rural area of Argentina, in children followed from age 7 to 12 years.
Key words: myopia, prevalence, rural, outdoors, myopia progression.
Baja prevalencia de miopía en niños de una población rural en Marcos Juárez, Argentina
Resumen
Objetivo: Este estudio fue desarrollado para evaluar la prevalencia y progresión de la miopía en niños que viven en una zona rural de Argentina.
Métodos: Se trata de un estudio de cohorte prospectivo sobre el error de refracción de niños de edad escolar. Los niños que asistían a todas las escuelas de Marcos Juárez se examinaron primero al ingresar a la escuela y 5 años después (de 11 a 12 años). El equivalente esférico (EE) se obtuvo bajo cicloplejía.
Resultados: En 2013, 347 niños fueron examinados y 283 de ellos estuvieron disponibles 5 años después (81%). La edad media al momento del segundo examen fue de 11,84 ± 0,36 años. El EE medio fue de +1,36 ± 0,83 D en 2013 y disminuyó significativamente a +1,07 ± 1,03 D en 2018 (un cambio general de -0,30 D, p <0,001). La prevalencia de miopía <-0,50 D fue baja (2,12% en 2013 y 3,53% en 2018) y no hubo casos de miopía alta <-5,00 D en ninguno de los períodos. La prevalencia de hipermetropía (> +2,00 D) disminuyó de 15,55% en 2013 a 9,54% en 2018, mientras que la prevalencia de emetropía e hipermetropía baja (-0,50 a +2,00 D) aumentó con el seguimiento (82,68% en 2013 a 86,92% en 2018). Hubo una incidencia muy baja de miopía en cinco años (1,44%).
Conclusión: Se detectó una baja prevalencia e incidencia de miopía en una zona rural de Argentina en niños seguidos de 7 a 12 años.
Palabras clave: miopía, prevalencia, rural, aire libre, progresión de la miopía.
Baixa prevalência de miopia em crianças de uma população rural em Marcos Juárez, Argentina
Resumo
Objetivo: Este estudo foi desenvolvido para avaliar a prevalência e a progressão da miopia em crianças que vivem em uma área rural da Argentina.
Métodos: Este foi um estudo de coorte prospectivo de erro refrativo em crianças em idade escolar. As crianças que freqüentavam todas as escolas em Marcos Juarez foram examinadas primeiro na entrada da escola e 5 anos depois (com 11-12 anos de idade). O equivalente esférico (EE) foi obtido sob cicloplegia.
Resultados: Em 2013, 347 crianças foram examinadas e 283 delas estavam disponíveis 5 anos depois (81%). A idade média no momento do segundo exame era de 11,84 ± 0,36 anos. O EE médio era +1,36 ± 0,83 D em 2013 e diminuiu significativamente para +1,07 ± 1,03 D em 2018 (uma variação geral de -0,30 D, p <0,001). A prevalência de miopia <-0,50 D foi baixa (2,12% em 2013 e 3,53% em 2018) e não houve casos de miopia alta <-5,00 D em nenhum dos períodos. A prevalência de hipermetropia (> +2,00 D) diminuiu de 15,55% em 2013 para 9,54% em 2018, enquanto a prevalência de emetropia e baixa hipermetropia (-0,50 para +2,00 D) aumentou com o acompanhamento (82,68% em 2013 para 86,92% em 2018). Houve uma incidência muito baixa de miopia em cinco anos (1,44%).
Conclusão: Uma baixa prevalência e incidência de miopia foi detectada em uma área rural da Argentina em crianças de 7 a 12 anos de idade.
Palavras-chave: miopia, prevalência, rural, ao ar livre, progressão da miopia.
INTRODUCTION
Myopia prevalence has been increasing worldwide in recent generations of children and adolescents1. The prevalence of myopia reaches values near 80% in the late adolescent population in some locations, as in Korea2 and Taiwan3, such that the demand for spectacles and contact lenses has become huge1, 4-11. High myopia has reached a prevalence of 10-20% at age 18 in several East and South-East Asian urban environments. It is expected that half of these myopic adolescents may have high-myopia macular complications, leading to impaired reading performance, when they reach their 50’s1, 12-13. This epidemic of myopia in East and South-East Asia is most probably environmental, produced by two main independent risk factors:7, 14 high academic load, with many hours of writing and reading printed material, and low outdoor exposure to daylight7, 12.
Typically, in rural environments with high outdoor exposure such as Nepal6,15, children and adolescents develop little or no myopia. Similarly in Argentina, a mainly European adult population16 of the province of Cordoba, has a low prevalence of myopia (13.5% in adults aged 40-60)17. It would be useful to study prospectively the prevalence of myopia in children and adolescents in locations with a low prevalence of myopia, since this would show how refractive error develops in humans under natural environments with limited exposure to myopia risk factors.
Marcos Juarez city is located in the southeast of Cordoba, where the main occupation involves agriculture with great economic development. The climatic conditions and the fertile land make it an excellent place to grow wheat, corn and soy. The nearest cities are around 30 km away, and between them, the land is 100% used for agriculture. In Marcos Juarez, children attend school either during the morning or the afternoon, 4 hours daily, and they spend the rest of the day mainly at outdoor activities. Most of them attend different clubs, where they play sports in outdoors environments. The present study was developed to evaluate the prevalence and progression of myopia, measured by cycloplegic autorefraction, in Marcos Juarez, in a sample of children followed at two time points (ages 6-7, at school entrance; and five years later, at the end of primary school).
MATERIALES AND METHODS
Study design, ethics and participants
This was a prospective school-based study, which involved the 6-7-year-old children residents in the city of Marcos Juarez, Cordoba Province, Argentina. Children were examined in June and July, 2013, during winter, in the first year of their primary school entrance; and then again, 5 years later, in their last year of primary education. Both examinations were part of an annual preventive campaign (“To see you better”), developed 23 years ago by the “Dr. Magnetto Vision Center” located in this city. This screening was approved by the local authorities of Cordoba Province, and carried out under the auspices of the Public Health Bureau of Marcos Juarez Department. The present study protocol was approved by the Ethics Committee of the Argentinian Council of Ophthalmology. One week before the ocular exam took place, each school sent a written informed consent as homework for the parents to allow the examination. In all schools of Marcos Juarez 302 children were first graders in 2018, of whom 283 (93.7%) gave consent for the exam (in 2013 there were 374 first graders, 347 available for exam, 92.7%). All data were maintained confidential except for the purpose of this publication, in accordance to the Declaration of Helsinki and Argentinian Federal Law. The city of Marcos Juárez has a stable population, with little migration, and according to the 2010 population census it had 27.004 inhabitants18.
Settings and procedures
The ocular exam took place at the building of the Deliberative Council of Marcos Juarez, and consisted in two days of work, scheduling children’s visits according to the schools at which they were enrolled. Two ophthalmologists measured visual acuity, projecting Snellen letters with an optotype projector at 5 meters (TOPCON, ACP-3, Tokyo, Japan). After this, another ophthalmologist instilled two cycles of cyclopentolate 1% drops and one of tropicamide 1%, at five-minute intervals, after an initial instillation of one drop of proparacaine 0.05% for topical anesthesia. After one hour, pupil dilation and pupillary reflex were examined to ensure the efficacy of cycloplegia, and cyclopentolate 1% was instilled again in the few cases that required it. Then cycloplegic auto-refraction was performed (±0.25 D) (TOPCON RM8000, Tokyo, Japan), and the fundus of the eye was examined.
Main outcomes and statistical evaluation
The mean of five cycloplegic refraction measurements was calculated, excluding outliers greater than 1 diopter of the mean value, and the spherical equivalent refraction (SER) was calculated as the sphere + ½ the cylinder value. For the purpose of reporting prevalence of refractive error, the present study followed the protocol of Refractive Error Studies in Children19: myopia was considered as the spherical equivalent refractive error <-0.50 dioptres (D), hyperopia as >+2.00 D, and the rest among -0.50 and +2.00 D were considered emmetropes. Parametric values were expressed as mean, standard deviations and range. The data were recorded in an Excel spreadsheet and converted to SPSS database (SPSS version 15, SPSS Inc., Chicago, IL, USA). Chi-square tests were performed to test proportions. Pearson correlation scatterplots, McNemar's chi-square tests for proportions and paired-sample t-tests for continuous variables were performed. The spherical equivalents of the right and left eyes were similar (Pearson correlation r = 0.85), so only right eyes are reported for the purpose of this study. A p value < 0.05 was taken as the cut-off for statistical significance.
RESULTS
In July 2013, the study involved 347 first grade children and 283 participated in the second examination five years later in August 2018 (81% of the original sample). At baseline these children were aged 6.84 ± 0.36 years, and at follow up they were aged 11.84 ± 0.36 years, and 49.5% were males. The mean SER decreased significantly from +1.36 ± 0.83 D in 2013 to +1.07 ± 1.03 D in 2018 (p < 0.001, an overall myopic shift of -0.30 dioptres). Kurtosis increased from 2.43 in 2013, to 7.94 in 2018. Skewness changed towards the myopic side from 0.12 in 2013, to -1.06 in 2018.
The prevalence of myopia < -0.50 D was low (2.12% in 2013 and 3.53% in 2018), and there were no cases of high myopia (<-5.00 D) in either exam period. The mean SER of the myopic cases increased from -1.38D in 2013 to -2.60D in 2018 (the mean progression in 5 years was low, at -1.23D change in the whole period). There was a very low incidence of myopia in five years (1.44%).
The prevalence of hyperopia (> +2.00 D) decreased from 15.20% in 2013, to 9.54% in 2018, while the prevalence of emmetropia + low hyperopia (between -0.50 and +2.00 D) increased with follow-up (Table 1, Chi Square, p = 0.036). The two distributions of refractive error are shown in Figure 1. It can be clearly seen that, although the prevalence of myopia did not change much, the distribution did have a slight myopic shift following the also slight decrease in mean SER.
Table 1. Prevalence of refractive error at both time points (n = 283). |
||
|
Year 2013 |
Year 2018 |
Myopia < -0.50 dioptres |
2.12% |
3.53% |
Emmetropia (-0.50 to +2.00 dloptres) |
82.68% |
86.92% |
Hyperopia > +2.00 dioptres |
15.20% |
9.54% |
(Chi Square p = 0.036) |
||
Figure 1. Histogram showing the distributions of spherical equivalent refractions, initially (dashed line) and after 5 years (solid line), showing slight loss of hyperopia without significant changes in myopia prevalence.
To further explore the change in refractive error between the times of examination, the mean SERs were compared by splitting the sample according to intervals of one diopter of refraction at baseline, from 0 to +3 dioptres. The analysis is shown in Table 2, where it can be seen that when baseline refractions were between plano and +1.00, the myopic shift was small and not significant (-0.16 dioptres); but when refractions at baseline were hyperopic (between +2.00 and +3.00 dioptres), the myopic shift significantly reached -0.52 dioptres. Figure 2 (a-c) shows a diagram of the refractive change for these different intervals of refractive error at baseline. It can be seen that most eyes having baseline SERs in the range of +1.00 to +2.00 D maintained stable refractions.
Table 2. Mean spherical equivalent refraction change when sample split by refractive error at baseline (D). |
|
|
|
|
|
Year 2013 |
Year 2018 |
Difference |
Student - p value |
Mean refraction at baseline from 0 to <+1.00 diopter (±SD) |
+0.56±0.27 |
+0.40±0.78 |
-0.16 |
0.112 |
Mean refraction at baseline from +1.00 to <+2.00 diopters (±SD) |
+1.40±0.27 |
+1.14±0.46 |
-0.26 |
<0.001 |
Mean refraction at baseline from +2.00 to <+3.00 diopters (±SD) |
+2.32±0.27 |
+1.80±0.58 |
-0.52 |
<0.001 |
DISCUSSION
The present study in a small city in the Argentinian Pampas shows a low prevalence, incidence or progression of myopia in children followed from school entrance to puberty. During the last 30 years, the prevalence of myopia has increased in many countries, as people have come to live in urban environments with low ambient lighting and high academic load7, 13. Locations where academic achievement and reading habits are intense, particularly in urban environments of East and South-East Asia, have produced an epidemic of myopia and high myopia7. In contrast, children in a rural small city, such as Marcos Juarez, are probably not subject to this myopigenic environment. So here we can have a picture of how refractive error might have developed in children under more ‘natural’ conditions —before people moved to highly developed urban environments, full of high buildings and having classrooms with low-intensity artificial ambient lights and high academic load.
The prevalence of myopia found in our study, at both time points, was as low as those in Nepal15 and Laos6-7, 20. Also, recent studies in Europe have shown low prevalence of myopia at ages 6-7, but not at ages 11-12. For example, the Northern Ireland Childhood Errors of Refraction (NICER) has found a prevalence of myopia of 1.9% at school entrance, and of 14.6% at age 12, higher than that of the present study21. Also, in a recent cross-sectional study of Polish schoolchildren, the prevalence of myopia was 2.0% at school entrance, but 14.36% at age 1222. The prevalence of myopia of 3.53% by ages 11-12, as found in the present study, is very low compared to those found in urban environments of East and South-East Asia23.
There were few early-onset myopic children in 2013, that were aged 6-7 at school entrance in the present study and they had a progression rate of -1.23 D in five years, or an average around -0.25 D per year. This rate of progression is very low, compared to that of same-aged children with early onset in urban Asian environments (≥1.00 D per year)24-25, suggesting further that environmental factors could influence the rate of progression7. The incidence of myopia was very low in the present study (1.44% over 5 years), compared with that found in children of the same age in Australia (14.0% over 5 years)26. These two last findings point to the probable importance of environmental interventions involving more outdoor exposure to treat both pre-myopic subjects near plano refractions and also children who have already become myopic.
To our knowledge, this is the first population-based study that shows prospectively the refractive error change after five years in a high-outdoor living environment. Interestingly, the mean refractive error at ages 6-7 was +1.37 dioptres –probably the end-point of the emmetropization mechanism, which is up to now believed to end by age 2-3 with little change thereafter27. But most interestingly, this mean refractive error decreased significantly after living for five years in Marcos Juarez as the children with higher amounts of hyperopia had significantly greater myopic shifts (Table 2 and Figure 2).
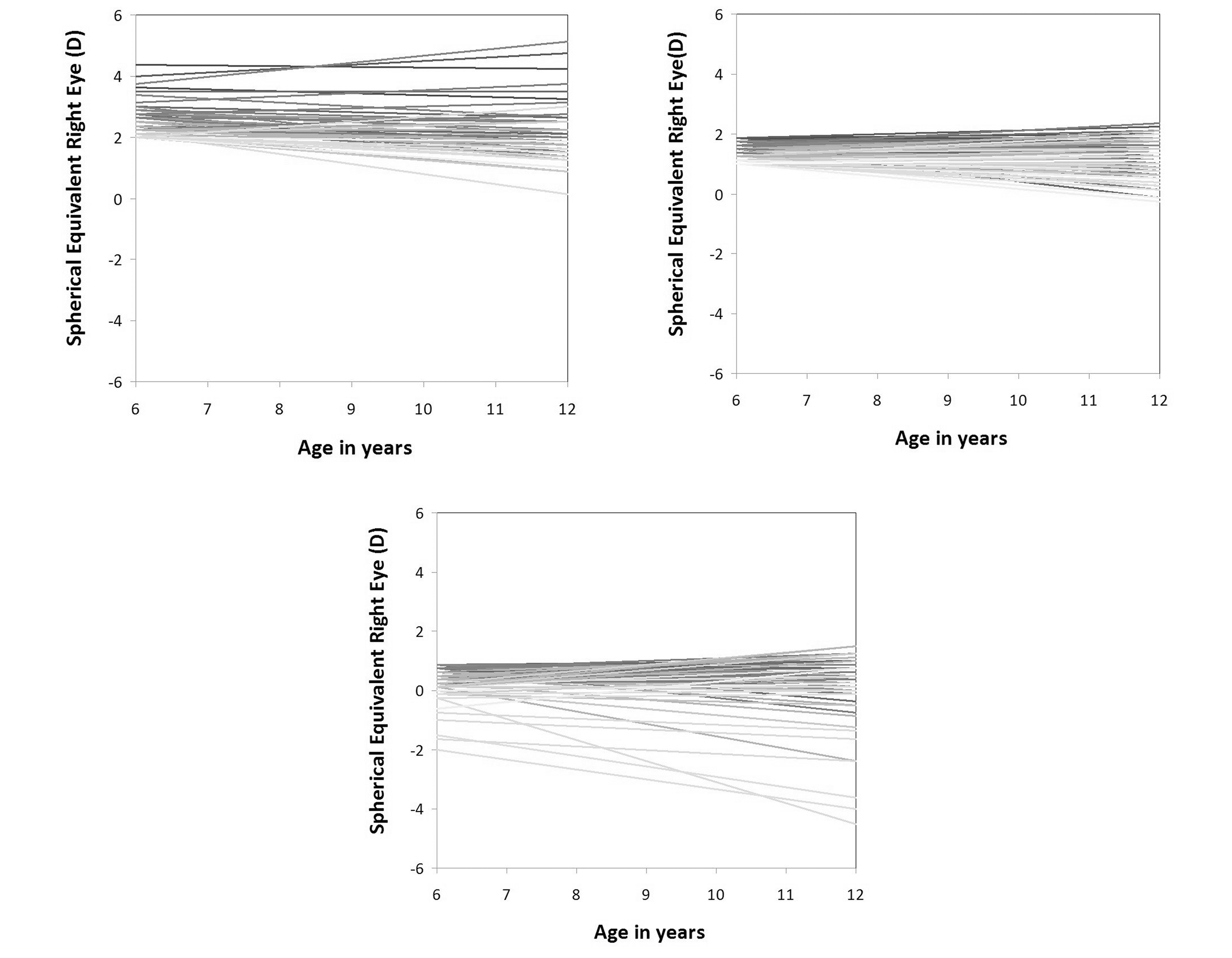
Figure 2. A-C) Refractive error at baseline and follow-up periods for each subject, according to groups of baseline refraction. A) Relatively high-hyperopia group. B) Intermediate-hyperopia group. C) Low-hyperopia group. Some high-hyperopic and some low-myopic eyes maintained stable refractions, while others underwent myopic shifts; in contrast, almost all eyes having baseline SERs in the range of +1.00 to +2.00 D maintained stable refractions.
This resembles the similar process of emmetropization that occurs during the first two years of life, when higher amounts of hyperopia are lost by increased axial elongation driven by hyperopic defocus signals28. Table 3 shows different cross-sectional and prospective studies involving children of same ages in locations with Caucasian populations where the prevalence of myopia has remained low15, 29-36. It can be clearly seen that there is a small tendency to develop lower amounts of mean SER as the children grow up during primary-school years, as we found prospectively in Marcos Juarez.
As we also see in Table 3, the prevalence of myopia is rather low in many locations. The projections for myopia prevalence to reach high levels by 2050, put forward by Holden et al.1, stand or fall on the strength of the underlying predictive models, rather than as established fact. If people continue living in high-outdoor environments, as do the children in the present study, these projections fortunately might not come true.
Table 3. Cross-sectional mean cycloplegic SER in different studies with low prevalence of myopia in children. |
||||
|
6-7 yo |
11-12 yo |
Myopia prevalence |
n |
Santiago de Chile36 |
+1.40 |
+0.70 |
12.5% |
5303 |
Generation R (Netherlands)32 |
- |
+0.74 |
11.4% |
6084 |
CLEERE Hispanic (USA)30 |
+0.84 |
+0.11 |
10.1% |
1116 |
CLEERE White (USA)30 |
+0.85 |
+0.59 |
10.1% |
1701 |
Tehran (Iran)35 |
+1.23 |
+0.70 |
7.2% |
557 |
Orinda (USA)29 |
+0.73 |
+0.50 |
5.0% |
530 |
Dezful (Iran)31 |
+1.28 |
+1.16 |
3.5% |
823 |
Mechi Zone (Nepal)15 |
+0.90 |
+0.70 |
3.0% |
5526 |
Marcos Juarez (Argentina) |
+1.37 |
+1.07 |
2.1% |
283 |
Paraguay34 |
- |
+1.76 |
1.2% |
444 |
Sydney (Australia)33 |
+1.27 |
+0.93 |
1.4% |
1281 |
Although there are differences in myopia prevalence in different ethnic groups, there is general agreement that these differences are not genetic in nature6, but due to different environmental conditions37 such as limited outdoor exposure and pressure for academic achievement5-7,14. The study of the genetic composition of our population showed that Argentineans are a mixture – with 80% European ancestry in autosomal and Y chromosomes16. The European genetic ancestry of this Argentinean population form Cordoba, with a very low prevalence of myopia in a probably high-outdoor-exposure environment, shows once more that myopia is probably largely an environmental disease6, 14. Besides, the few early onset in our study had a very low rate of progression, contrasting with the more than 1 D progression per year in similarly-aged children in Asia24-25.
The amount of time spent at school by all these children in Marcos Juarez was 4 hours. During the rest of the daytime, children in this city mostly play outdoors sports like football, soccer, rugby, hockey or tennis – sports activities in which distance vision and psychomotor activity are relevant. In addition, Marcos Juarez city is a small town with low buildings (not higher than 3 or 4 floors), where children move on foot or by bicycle. It is possible that this visual behavior with high outdoor exposure could also affect myopia progression as seen in the progression of the few early-onset myopes that we studied. Concerning academic achievement, Argentina is well known for supporting public education (85% are public schools) and having a high rate of literacy (99%)18. However, our country does not rank well in the PISA tests38; and although primary and secondary education are compulsory, there is a high rate of school dropout (50%)39, and only 20% of the population has a tertiary diploma40.
One important aspect to remark in this study is the use of cycloplegia with cyclopentolate and tropicamide, obtaining an accurate value of spherical equivalent refraction in children that could otherwise accommodate their hyperopic refractive error without cycloplegia. The principal drawbacks of this study are the lack of a questionnaire about time outdoors and reading habits, and the fact that no biometric data were obtained for these children. Future follow-ups will be adding these to the assessment of refractive error in children from Marcos Juarez.
CONCLUSIONS
In conclusion, we have presented data showing that the prevalence, incidence and progression of myopia are very low in this location –in 6- to 12-year-old children from a population-based study, in which there is clustering of refractions and a slight myopic shift in mean spherical equivalent in the follow-up during primary school-years. Future prospective population studies, comparing different visual behaviors, will increase the knowledge of the worldwide myopia epidemic and its causal factors.
REFERENCES
1. Holden BA, Fricke TR, Wilson DA et al. Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050. Ophthalmology 2016; 123: 1036-1042.
2. Kim EC, Morgan IG, Kakizaki H et al. Prevalence and risk factors for refractive errors: Korean National Health and Nutrition Examination Survey 2008-2011. PloS One 2013; 8: e80361.
3. Lin LL, Shih YF, Hsiao CK et al. Epidemiologic study of the prevalence and severity of myopia among schoolchildren in Taiwan in 2000. J Formos Med Assoc 2001; 100: 684-691.
4. Foster PJ, Jiang Y. Epidemiology of myopia. Eye (Lond) 2014; 28: 202-208.
5. French AN, Ashby RS, Morgan IG, Rose KA. Time outdoors and the prevention of myopia. Exp Eye Res 2013; 114: 58-68.
6. Morgan I, Rose K. How genetic is school myopia? Prog Retin Eye Res 2005; 24: 1-38.
7. Morgan IG, French AN, Ashby RS et al. The epidemics of myopia: Aetiology and prevention. Prog Retin Eye Res 2018; 62: 134-149.
8. Morgan IG, He M, Rose KA. Epidemic of pathologic myopia: what can laboratory studies and epidemiology tell us? Retina 2017; 37: 989-997.
9. Morgan IG. What public policies should be developed to deal with the epidemic of myopia? Optom Vis Sci 2016; 93: 1058-1060.
10. Theophanous C, Modjtahedi BS, Batech M et al. Myopia prevalence and risk factors in children. Clin Ophthalmol 2018; 12: 1581-1587.
11. Hsu CC, Huang N, Lin PY et al. Prevalence and risk factors for myopia in second-grade primary school children in Taipei: a population-based study. J Chin Med Assoc 2016; 79: 625-632.
12. Morgan IG, Ohno-Matsui K, Saw SM. Myopia. Lancet 2012; 379: 1739-1748.
13. Pan CW, Ramamurthy D, Saw SM. Worldwide prevalence and risk factors for myopia. Ophthalmic Physiol Opt 2012; 32: 3-16.
14. Morgan IG, Rose KA. Myopia: is the nature-nurture debate finally over? Clin Exp Optom 2019; 102: 3-17.
15. Pokharel GP, Negrel AD, Munoz SR, Ellwein LB. Refractive error study in children: results from Mechi Zone, Nepal. Am J Ophthalmol 2000; 129: 436-444.
16. Corach D, Lao O, Bobillo C, van Der Gaag K. Inferring continental ancestry of argentineans from Autosomal, Y-chromosomal and mitochondrial DNA. Ann Hum Genet 2010; 74: 65-76.
17. Sanchez V IR, Latino SG, Torres VE et al. Prevalence of refractive errors in Villa Maria, Córdoba, Argentina. Eye Science 2016; 31: 68-77.
18. Argentina. Instituto Nacional de Estadística y Censo (INDEC). Censo Nacional de Población, Hogares y Viviendas 2010 [en línea]. https://www.indec.gob.ar/indec/web/Nivel4-Tema-2-41-135
19. Negrel AD, Maul E, Pokharel GP et al. Refractive error study in children: sampling and measurement methods for a multi-country survey. Am J Ophthalmol 2000; 129: 421-426.
20. Casson RJ, Kahawita S, Kong A et al. Exceptionally low prevalence of refractive error and visual impairment in schoolchildren from Lao People’s Democratic Republic. Ophthalmology 2012; 119: 2021-2027.
21. McCullough SJ, O'Donoghue L, Saunders KJ. Six year refractive change among white children and young adults: evidence for significant increase in myopia among white UK children. PloS One 2016; 11: e0146332.
22. Czepita D, Zejmo M, Mojsa A. Prevalence of myopia and hyperopia in a population of Polish schoolchildren. Ophthalmic Physiol Opt 2007; 27: 60-65.
23. Morgan IG, French AN, Rose KA. Risk factors for myopia: putting causal pathways into a social context. En: Ang M, Wong TY (eds.). Updates on myopia: a clinical perspective. Singapore: Springer Nature, 2020.
24. Holden B, Sankaridurg P, Smith E et al. Myopia, an underrated global challenge to vision: where the current data takes us on myopia control. Eye (Lond) 2014; 28: 142-146.
25. Sankaridurg PR, Holden BA. Practical applications to modify and control the development of ametropia. Eye (Lond) 2014; 28: 134-141.
26. French AN, Morgan IG, Burlutsky G et al. Prevalence and 5- to 6-year incidence and progression of myopia and hyperopia in Australian schoolchildren. Ophthalmology 2013; 120: 1482-1491.
27. Morgan IG, Rose KA, Ellwein LB. Refractive error study in children survey group. Is emmetropia the natural endpoint for human refractive development? An analysis of population-based data from the Refractive Error Study in Children (RESC). Acta Ophthalmol 2010; 88: 877-784.
28. Mutti DO, Mitchell GL, Jones LA et al. Axial growth and changes in lenticular and corneal power during emmetropization in infants. Invest Ophthalmol Vis Sci 2005; 46: 3074-3080.
29. Zadnik K, Mutti DO, Friedman NE, Adams AJ. Initial cross-sectional results from the Orinda Longitudinal Study of Myopia. Optom Vis Sci 1993; 70: 750-758.
30. Twelker JD, Mitchell GL, Messer DH et al. Children’s ocular components and age, gender, and ethnicity. Optom Vis Sci 2009; 86: 918-935.
31. Fotouhi A, Hashemi H, Khabazkhoob M, Mohammad K. The prevalence of refractive errors among schoolchildren in Dezful, Iran. Br J Ophthalmology 2007; 91: 287-292.
32. Tideman JWL, Polling JR, Vingerling JR et al. Axial length growth and the risk of developing myopia in European children. Acta Ophthalmol 2018; 96: 301-309.
33. Ojaimi E, Rose KA, Morgan IG et al. Distribution of ocular biometric parameters and refraction in a population-based study of Australian children. Invest Ophthalmol Vis Sci 2005; 46: 2748-2754.
34. Carter MJ, Lansingh VC, Schacht G et al. Visual acuity and refraction by age for children of three different ethnic groups in Paraguay. Arq Bras Oftalmol 2013; 76: 94-97.
35. Hashemi H, Fotouhi A, Mohammad K. The age- and gender-specific prevalences of refractive errors in Tehran: the Tehran Eye Study. Ophthalmic Epidemiol 2004; 11: 213-225.
36. Maul E, Barroso S, Munoz SR et al. Refractive Error Study in Children: results from La Florida, Chile. Am J Ophthalmol 2000; 129: 445-454.
37. Hobday R. Myopia and daylight in schools: a neglected aspect of public health? Perspect Public Health 2016; 136: 50-55.
38. Morgan IG, Rose KA. Myopia and international educational performance. Ophthalmic Physiol Opt 2013; 33: 329-338.
39. Scasso MG. ¿Cuántos jóvenes terminan la educación secundaria en la Argentina?: cómo monitorear las metas de universalización de la educación secundaria. Propuesta Educativa 2018; 49: 32-47.
40. García de Fanelli AM. Rendimiento académico y abandono universitario: modelos, resultados y alcances de la producción académica en la Argentina. Rev Arg Edu Sup 2014; 6: 9-38.